Advocacy 2026

Advocacy – it’s not a bad word.
There are three major types of advocacy: self-advocacy, individual advocacy, and systems advocacy.
Self advocacy means identifying your unique voice and creating your “brand.” It’s a variation of having that 30 second elevator pitch ready to go. Individual advocacy means learning how to advocate for others, as mentors and sponsors, elevating the presence and inclusion of others. Systems advocacy means knowing how to assert yourself into decision-making processes and using management strategies to make change happen.
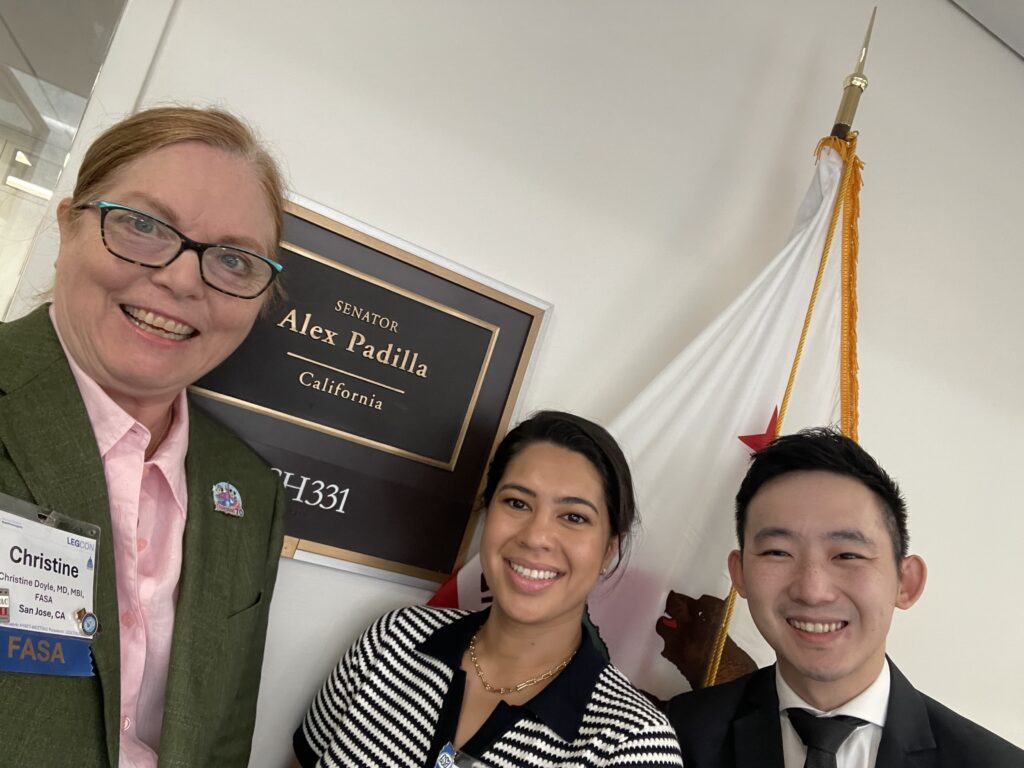
That said, I just returned from the ASA’s Legislative Conference (LEGCON) last week. This is definitely a systems advocacy event. Leading the California Society of Anesthesiologists (CSA) delegation was fun and exhausting. We visited 29 offices with a total of 16 people, including 6 residents and medical students.
I also got to visit my friend and former Assemblymember, Evan Low. He’s now working at the Victory Fund.


Meme-worthy photos
While at the CSA Annual Meeting in April, we noted that the presidents of the three largest component societies (California, New York, and Texas) all had a woman as President. As far as we know, this is the first time this has occurred.
In order to commemorate the event, we took a lot of photos. Dr. Stacey Watt (New York President) thought it would be fun if they posted like Charlie’s Angels… with airway equipment in their hands. I took that original photo, against the CSA backdrop, and edited it to create “Anesthesia Angels.”
It was a big hit. Now to figure out what other photos we can use for the women of the ASA.
References for CSA 2026 Annual Meeting: Scheduling and AI
References cited in the presentation:
- NASA. What is Artificial Intelligence? [Internet]. [cited 2026 Apr 6]. Available from: https://www.nasa.gov/what-is-artificial-intelligence/
- Oremus W. He spent decades perfecting his voice. Now he says Google stole it. The Washington Post [Internet]. 2026 Feb 15 [cited 2026 Feb 15]. Available from: https://www.washingtonpost.com/technology/2026/02/15/david-greene-google-ai-podcast/
- Fadel L. Former “Morning Edition” host accuses Google of stealing his voice for AI product. NPR [Internet]. 2026 Feb 17 [cited 2026 Apr 2]. Available from: https://www.npr.org/2026/02/17/nx-s1-5716055/former-morning-edition-host-accuses-google-of-stealing-his-voice-for-ai-product
- Chayka K. Is A.I. Art Stealing from Artists? The New Yorker [Internet]. 2023 Feb 10 [cited 2026 Mar 31]. Available from: https://www.newyorker.com/culture/infinite-scroll/is-ai-art-stealing-from-artists
- Generative AI is a marvel. Is it also built on theft? The Economist [Internet]. [cited 2026 Mar 31]. Available from: https://www.economist.com/business/2024/04/14/generative-ai-is-a-marvel-is-it-also-built-on-theft
- Revealed: how academics are being deepfaked on TikTok and Instagram to promote supplements – Full Fact [Internet]. 18:45:23.581133+00:00 [cited 2026 Feb 15]. Available from: https://fullfact.org/health/academics-deepfaked-tiktok-wellness-nest/
- Myers SL, Callahan A, Rosenbluth T. The Doctors Are Real, but the Sales Pitches Are Frauds. The New York Times [Internet]. 2025 Sep 5 [cited 2026 Feb 17]. Available from: https://www.nytimes.com/2025/09/05/technology/ai-doctor-scams.html
- Whyte J. AMA CEO: Deepfake doctors are a threat to public health. STAT [Internet]. 2026 Feb 17 [cited 2026 Feb 17]. Available from: https://www.statnews.com/2026/02/17/deepfake-doctors-scam-ama/
- Harris T, Blakely R. Publisher under fire after ‘fake’ citations found in AI ethics guide [Internet]. 2025 [cited 2026 Feb 15]. Available from: https://www.thetimes.com/uk/science/article/ai-ethics-guide-citations-nsnjmz25b
- Klee M. AI is Inventing Academic Papers That Don’t Exist — And They’re Being Cited in Real Journals. Rolling Stone [Internet]. 2025 Dec 17. Available from: https://www.rollingstone.com/culture/culture-features/ai-chatbot-journal-research-fake-citations-1235485484/
- Walters WH, Wilder EI. Fabrication and errors in the bibliographic citations generated by ChatGPT. Sci Rep. 2023 Sep 7;13(1):14045. doi:10.1038/s41598-023-41032-5
- Anand BN, Wu A. The Gen AI Playbook for Organizations. Harvard Business Review [Internet]. 2025 Nov 1 [cited 2026 Apr 3]. Available from: https://hbr.org/2025/11/the-gen-ai-playbook-for-organizations
Related Reading (in no particular order):
- Marr B. Forbes [Internet]. [cited 2026 Apr 6]. AI: Overhyped Fantasy Or Truly The Next Industrial Revolution? Available from: https://www.forbes.com/sites/bernardmarr/2024/08/15/ai-overhyped-fantasy-or-truly-the-next-industrial-revolution/
- Walsh D. A new look at the economics of AI | MIT Sloan [Internet]. 2025 [cited 2026 Apr 6]. Available from: https://mitsloan.mit.edu/ideas-made-to-matter/a-new-look-economics-ai
- Built In [Internet]. [cited 2026 Apr 1]. What Is Deep Learning and How Does It Work? Available from: https://builtin.com/machine-learning/deep-learning
- Choudhry D. Using AI to create work schedules significantly reduces physician burnout, study shows [Internet]. ASA; 2022 [cited 2026 Mar 27]. Available from: https://www.asahq.org/about-asa/newsroom/news-releases/2022/01/using-ai-to-create-work-schedules-significantly-reduces-physician-burnout
- Gen AI Won’t Make Your Employees Experts. Harvard Business Review [Internet]. 2026 Mar 1 [cited 2026 Mar 8]. Available from: https://hbr.org/2026/03/gen-ai-wont-make-your-employees-experts
- Bedard J, Kropp M, Hsu M, Karaman OT, Hawes J, Kellerman GR. When Using AI Leads to “Brain Fry.” Harvard Business Review [Internet]. 2026 Mar 5 [cited 2026 Mar 8]. Available from: https://hbr.org/2026/03/when-using-ai-leads-to-brain-fry
- Medscape [Internet]. [cited 2026 Apr 6]. Should Doctors Strike to Limit AI Use at Work? Available from: https://www.medscape.com/viewarticle/should-doctors-strike-protect-their-jobs-against-ai-2026a10009vg
- Stackpole T. LLMs Are Manipulating Users with Rhetorical Tricks. Harvard Business Review [Internet]. 2026 Mar 18 [cited 2026 Apr 7]. Available from: https://hbr.org/2026/03/llms-are-manipulating-users-with-rhetorical-tricks
- Chatterjee R. AI in the mental health care workforce is met with fear, pushback — and enthusiasm. NPR [Internet]. 2026 Apr 7 [cited 2026 Apr 8]. Available from: https://www.npr.org/2026/04/07/nx-s1-5771707/mental-health-care-workforce-artificial-intelligence-ai
- Kannarkat JT, Abraham PA, King JS. Workflow Blocking in Clinical Care: The Usability Gap Beyond Information Blocking. JAMA. 2026 Apr 8. doi:10.1001/jama.2026.3249
- Ullah W, MD. Opinion | Replace Yourself With AI, CEO Katz [Internet]. 2026 [cited 2026 Apr 10]. Available from: https://www.medpagetoday.com/opinion/second-opinions/120627
ASA Candidacy
This past October, I ended up tossing my hat in the ring to run for the Vice-Speaker position at the American Society of Anesthesiologists (ASA), for election in October 2026.
The Vice-Speaker and Speaker serve as the parliamentarians for our Board of Directors and House of Delegates meetings. The role includes ensuring that everyone’s voice is heard and that debate is robust but fair to all attendees.
I was the Vice-Speaker and Speaker for the California Society of Anesthesiologists (CSA) between 2011-2018, prior to becoming President-Elect and President.
My campaign-specific website is at drdoyle4asa.com. Check it out!

The frustrations of plugins
Posting, so that someone else won’t have to work quite as hard to solve this problem.
I created a new website, installed the Wordfence plugin (version 8.1.2), got my license key for the site, installed it, and I keep getting the “Wordfence installation is incomplete” with the banner across the top of the screen. Even after entering the license key repeatedly.
Opening the console did not show any errors.
I cleared my cache, turned off all my other plugins, rebooted both Chrome and computer. Nothing changed.
Finally, I deleted the Wordfence plugin with all of the associated data and tables, and then reinstalled it. And it immediately started working.
Tracing my Italian family
The family has long talked about visiting Italy and our grandparents’ hometown. With changes in Italian law, one can claim (reclaim?) Italian citizenship through either the paternal or maternal line. So, down the rabbit hole to collect a variety of records and see what we all might be able to do.
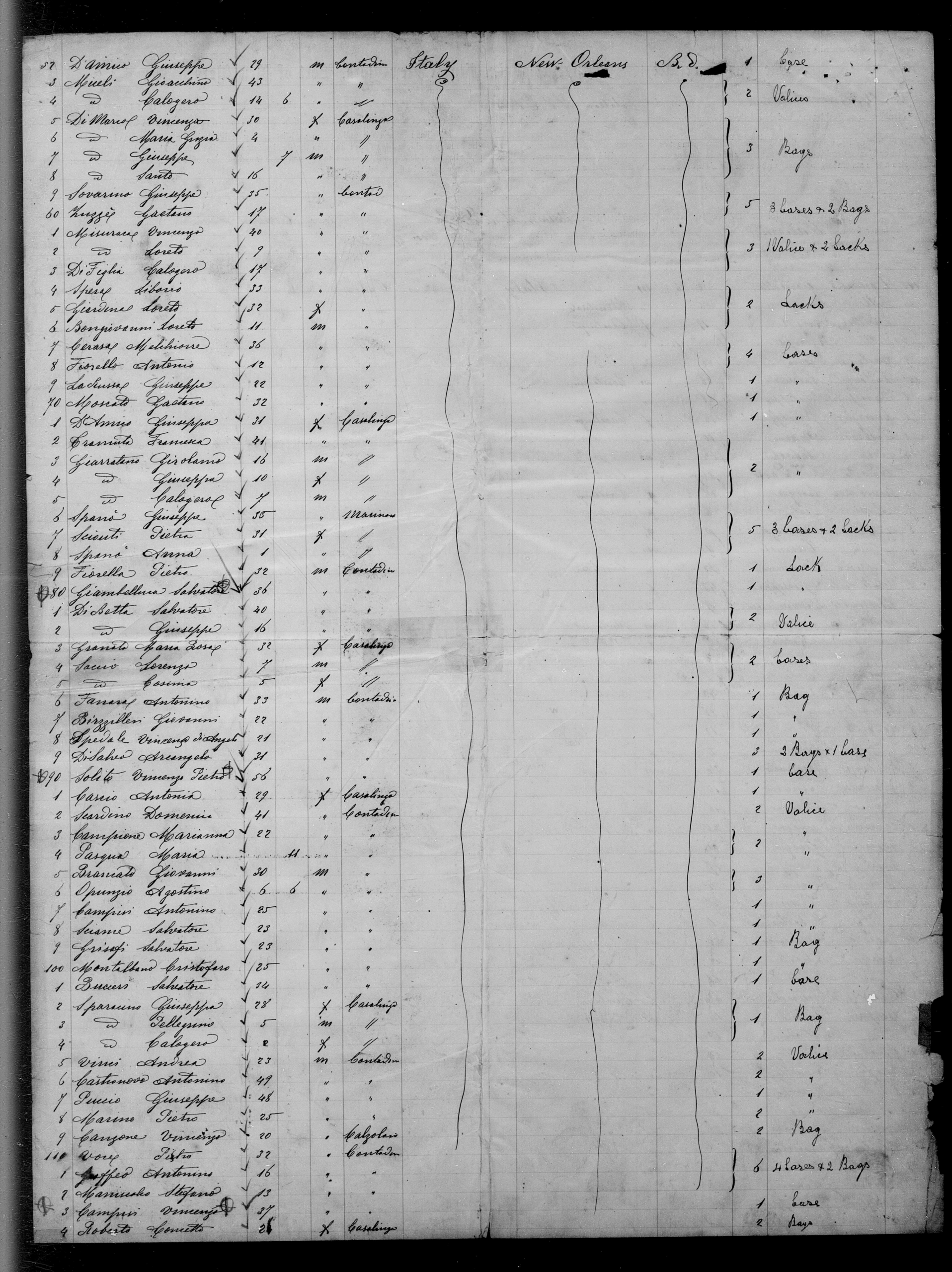
Step 1: See if we can find the ship manifests for when each of my grandparents came to the US. We know the year for each of them. Family lore indicated that Pappa, at least, came in through New Orleans. But we didn’t know where Mamma came in — New Orleans or New York or another port.
We found Pappa on the SS Plata, which went from Palermo to New Orleans in 1891. And then Mamma on the SS Spartan Prince, from Naples to New York in 1898 with her mother and sister and cousin. All of these records are difficult to read.
Step 2: Pull up the copy of the marriage license that I made back in med school. The Omaha public library has a great family history section, and I found that it was a double wedding with one of her sisters. The two licenses also gave me a bunch of other family names.
Step 3: Figure out if either of them were naturalized citizens. This is the hard step, because before 1906, there was no central process or location for records. Naturalization could happen in local, district, state, or federal courts. And most of this is not available on-line. Notations on Census records may or may not be accurate. So there may be a trip to Omaha or the National Archives in Kansas City in our future.
Step 4: Verify all of the US Census records, through 1950 (the most recent year that’s available). This has been the most interesting yet tricky thing, because the family name has been spelled 4 different ways between 1900 and 1950. Pappa’s name is 4 different spellings, and Mamma’s is 3. I finally found them in the 1950 census by searching for their address!
Step 5: Now the hard part – finding records in Italy. This requires professional help. And time.
Harassment, Incivility, and Disrespect references
This presentation has appeared in various formats at various meetings, and the reference list has changed slightly as new information is published. The meetings include: CSA Winter Seminar 2025 (January 2025), ASA ADVANCE (January 2025), Vituity Partnership (September 2025), ASA Annual Meeting (October 2025), Post-Graduate Assembly (PGA, December 2025), ASA ADVANCE (January 2026). Most of these are journal articles, but there are some from the lay media.
ASA. Statement on Harassment, Incivility, and Disrespect [Internet]. 2024 [cited 2025 Jan 12]. Available from: https://www.asahq.org/standards-and-practice-parameters/statement-on-harassment-incivility-and-disrespect
Afonso AM, Cadwell JB, Staffa SJ, Zurakowski D, Vinson AE. Burnout Rate and Risk Factors among Anesthesiologists in the United States. Anesthesiology [Internet]. 2021 May 1 [cited 2021 Aug 20];134(5):683–96. Available from:
https://pubs.asahq.org/anesthesiology/article/134/5/683/115466/Burnout-Rate-and-Risk-Factors-among
Davis K, Pinto JK. The Corruption of Project Governance Through Normalization of Deviance. IEEE Transactions on Engineering Management [Internet]. 2024 [cited 2024 Jan 30];71:2447–61. Available from: https://ieeexplore.ieee.org/document/9826419
DeMaria, Samuel. The Invisible Cut: Incivility’s Silent Toll on Healthcare. 2025.
ISBN: 979-8294912680.
Hastie MJ, Mittel A, Raman V, Szokol J, Whittington R, Bustillo M, et al. Sexual Harassment in Academic Anesthesiology: A Survey of Prevalence, Sources, Impact, and Recommendations. Anesthesia & Analgesia [Internet]. 2022 Mar 18 [cited 2025 Jan 8];10.1213/ANE.0000000000007282. Available from: https://journals.lww.com/anesthesia-analgesia/fulltext/9900/sexual_harassment_in_academic_anesthesiology__a.1091.aspx
Lautenberger D, Dandar V, Zhou Y. AAMC. 2022 [cited 2022 Aug 8]. Understanding and Addressing Sexual Harassment in Academic Medicine. Available from: https://www.aamc.org/data-reports/faculty-institutions/report/understanding-and-addressing-sexual-harassment-academic-medicine
Lautenberger DM, Dandar VM. The State of Women in Academic Medicine 2023-2024: Progressing Toward Equity. Washington, DC: AAMC; November 2024. Available from: https://www.aamc.org/data-reports/faculty-institutions/report/state-women-academic-medicine
Ligibel JA, Goularte N, Berliner JI, et al. Well-Being Parameters and Intention to Leave Current Institution Among Academic Physicians. JAMA Network Open. 2023;6(12):e2347894. doi:10.1001/jamanetworkopen.2023.47894
Lin DM, Lane-Fall MB, Lea JA, Reede LJ, Gomes BD, Xia Y, et al. Workplace Violence Pervasiveness in the Perioperative Environment: A Multiprofessional Survey. The Joint Commission Journal on Quality and Patient Safety [Internet]. 2024 Nov 1 [cited 2025 Jan 12];50(11):764–74. Available from: https://www.sciencedirect.com/science/article/pii/S1553725024002320
Mashour GA. This Is Not Acceptable. ASA Monitor [Internet]. 2023 Apr 1 [cited 2023 Apr 17];87(4):34. Available from: https://doi.org/10.1097/01.ASM.0000925020.07308.aa
Muse IO, Markowitz SD, Doyle CA, Lin DM. ASA Statement on Harassment, Incivility, and Disrespect: Why, How, What…Why Now? ASA Monitor. 2025 Feb;89(2).
Rabin RC. Hundreds Sue Virginia Hospital and Executives Over Unneeded Surgeries. The New York Times [Internet]. 2025 Dec 30 [cited 2026 Jan 19]; Available from: https://www.nytimes.com/2025/12/29/health/chesapeake-hospital-lawsuit-perwaiz.html
Spitzer Y, Kraus M, Doyle CA. We’re #1… and That’s Bad: Anesthesiology Has the Highest Rates of HID. ASA Monitor [Internet]. 2025 Nov [cited 2025 Oct 23];89(11):12. Available from: https://journals.lww.com/monitor/fulltext/2025/11000/we_re__1____and_that_s_bad__anesthesiology_has_the.3.aspx
Graduation!
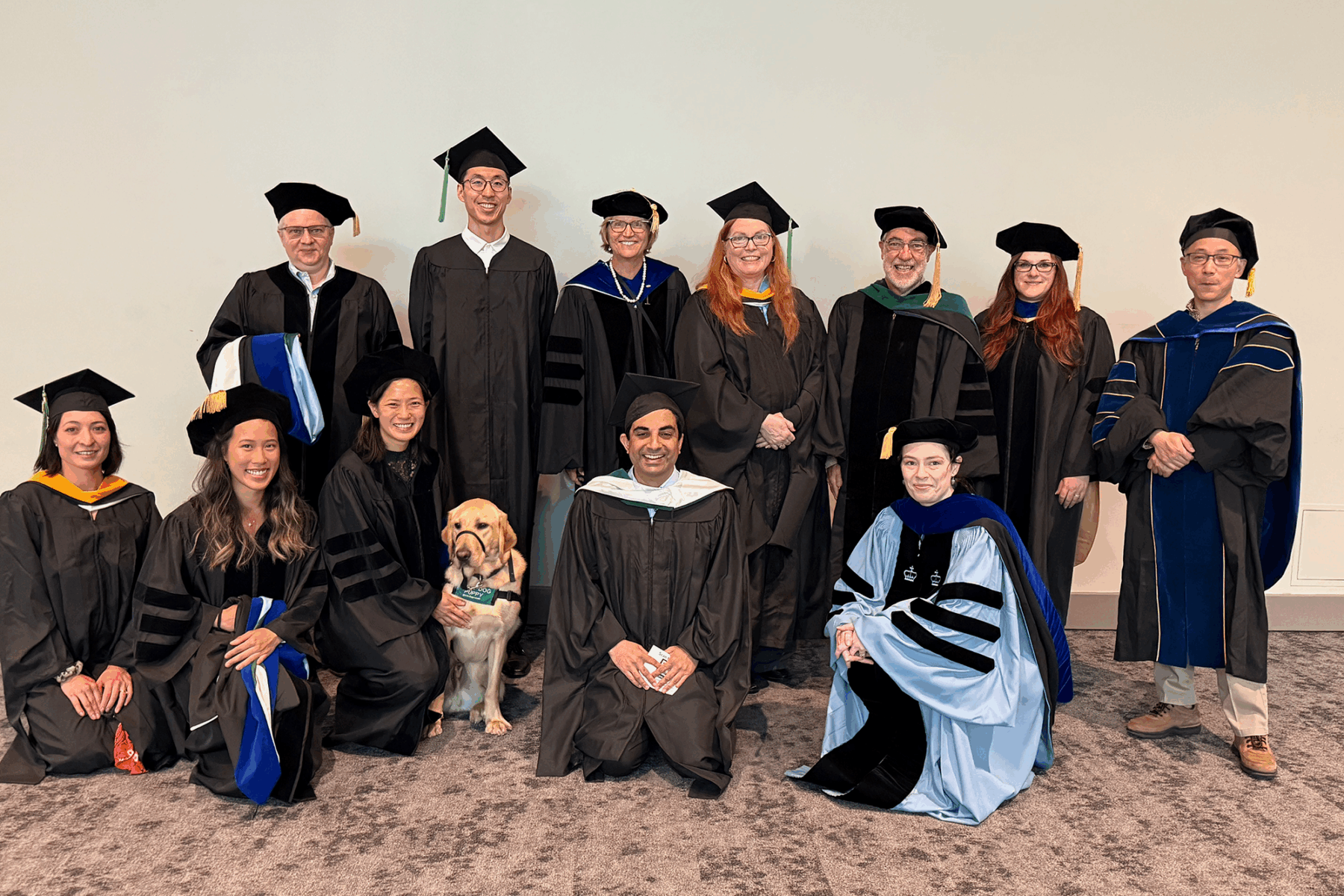
It’s official, I now have my Masters in Biomedical Informatics.
Commencement was June 6th, but the quarter didn’t end until the 20th, so grades posted a week or so later, at which point I could truly say I was done.
Our trip to Portland for commencement was a lot of fun. We had a chance to catch up with various folks who have moved there from the Bay Area over the years, and explore the area. It’s a place we definitely would like to visit again.

BMI 525 – Graph Exploration and Brief
Christine Doyle
May 5, 2025
TYPE OF GRAPH:
Bar Chart – aka Column Chart
DATA:
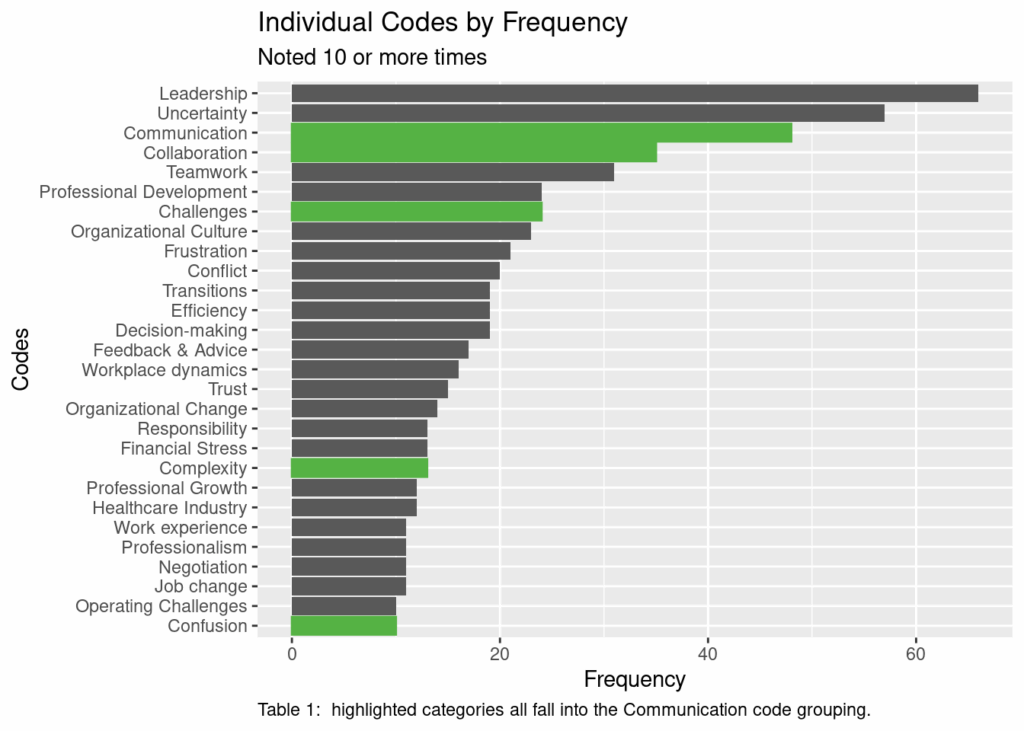
This data set was gathered as a part of a qualitative project involving interviews about organizational behavior. The individual concepts have been grouped into larger code groups. This table shows the most frequently identified concepts, and then specifically highlights the multiple concepts that are grouped into “Communication.”
Representation Description:
Bar charts display categorical information on one axis with continuous information on the other axis. The categorical variable may be random or ordered. The ordered variable may be sorted alphabetically or by number or by ascending or descending order based on the other variable. Typical categories might include a graph that has days of the week or locations on one axis (most often the x-axis) against the number of times something falls into that category on the second axis (most often the y-axis). The x-axis and y-axis typically will intersect at the bottom left corner of the chart. If the values are both positive and negative, the axis will be in the center. If the values are all negative, the axis will be at the top.
Bar charts may be oriented with the categorical variable either across the x-axis or y-axis. The orientation of the bar determines if it’s called horizontal or vertical. Horizontal charts have the categorical variable down the y-axis, and are often selected when there are long category labels or a large number of categories.
Bar charts may be grouped or stacked to provide information about two or more categorical variables. Grouped bars may be seen when comparing variable changes between two groups, for example, sales over time. Grouped bars can be easy to use with both positive and negative values. Stacked bars are more often seen when comparing both totals and proportions, particularly looking at change over time or comparison between the different primary categories. Stacked bars are more difficult to use if values are both positive and negative. Stacked bars may also be normalized to the same total height so that the sub-bars become the proportion of that secondary variable.
The bar chart is the most frequently used visualization for non-scientific audiences (i.e., newspaper/press, financial, and government/organizational).
A histogram is not the same as a bar chart, as it is two continuous variables, with one of them divided into groups, although it does look somewhat similar. A line chart is closely related to a bar chart, but implies a continuous progression.
How to Read a Bar Chart:
Simple bar charts should be examined for the order of the categorical variable — is it based on time, based on frequency, or based on something else. This will facilitate understanding of the overall data. Grouped or stacked bar charts should also be examined for the order of the first categorical variable, again looking at time or frequency or something else. If the data is not ordered by time, generally the first categorical variable will be presented in ascending or descending order, and the other variables will remain paired to the first.
Presentation Tips:
Interactivity: Bar charts are not often seen in an interactive presentation. When they are, the goal is to provide additional information about a given category when you select or hover over a particular selection.
Annotation: Annotation showing the exact value of a given variable may be presented overlaying or adjacent the bar. This can facilitate distinguishing between variables with similar amounts, particularly if the scale is condensed and if you are showing stacked bar charts where it is harder to appreciate changes in size of the bar.
Color: Color is often used to distinguish between the different categorical variables. It is most helpful for grouped or stacked bar charts, but can also be helpful in highlighting a specific category or category group.
Composition: The main arrangement decision is how the primary categorical variable is sorted. Dates and times are frequent choices, and may include years, months, days of the week, quarters of the year, etc. Ordering by frequency (either ascending or descending) is also a common arrangement.
Variations and Alternatives
As mentioned above, both grouped and stacked bar charts are variations of the simple bar chart. Depending on the data and time definitions, one might also consider a Sankey diagram.
How to Create it
code_freq <- read_csv(“data/CodeFrequency4Ranalysis1.csv”, col_types = cols()) code_freq <- code_freq %>% janitor::clean_names()
basic_plot = ggplot(code_freq, aes(x=frequency, y=reorder(code, +frequency))) + geom_col() + labs(x = “Frequency”, y = “Codes”) + ggtitle(“Individual Codes by Frequency”, subtitle = “Noted 10 or more times”) + scale_color_hue(c=20) + geom_col(data = subset(code_freq, code_group == “Communication”), color = “#55b244”, fill = “#55b244”) + theme(plot.caption = element_text(hjust = 0)) + # set the left align here labs(caption = “Table 1: highlighted categories all fall into the Communication code grouping.”)
###
Selling Your Hospital, Part 2
This post was originally published on the California Society of Anesthesiologist’s (CSA) webpage on March 7, 2016 With their website rebuild, the archives were not posted.
Home » CSA Online First » Christine Doyle » Selling Your Hospital, Part 2
Selling Your Hospital, Part 2
Mar 07, 2016 by Christine Doyle, M.D.
tags: hospitals

Between the initial announcement of the DCHS sale in October 2014, the conditional approval by the Attorney General on February 20, 2015, and Prime’s withdrawal of its offer on March 10, 2015, we held many meetings. Prime’s operations team visited on several occasions to review our processes and make suggestions. We started implementing some of them immediately, and others later.
 Probably the most important factor that changed was our attitude. We learned how truly important our documentation was for the hospital’s ability to bill for services. We learned about how coders do their work, even if we will never actually do it, so that we could help make their jobs easier. Our medical staff president spent hours one-on-one with our admitting physicians, showing them the difference a single word could make. Most of us had no idea, for example, that “urosepsis” wasn’t a valid diagnosis according to CMS. This information brought secondary benefits as well, as the ICD-10 transition became a non-issue for us.
Probably the most important factor that changed was our attitude. We learned how truly important our documentation was for the hospital’s ability to bill for services. We learned about how coders do their work, even if we will never actually do it, so that we could help make their jobs easier. Our medical staff president spent hours one-on-one with our admitting physicians, showing them the difference a single word could make. Most of us had no idea, for example, that “urosepsis” wasn’t a valid diagnosis according to CMS. This information brought secondary benefits as well, as the ICD-10 transition became a non-issue for us.
Our Geometric Mean Length of Stay (GMLOS), which started out 1.5 days over the target, was reduced to 0.1 days over the target within nine months. Although the actual increase in revenue was not known to us, it was clear that we were appropriately aligning our documentation with what was required by CMS.
We also looked long and hard at our expenses. A mitigation plan, aimed to reduce those expenses, was enacted in April. It was not without controversy, nor was it without revision. Key issues included inaccurate job titles, descriptions, and an overemphasis on confidentiality, leading to crucial positions being eliminated (i.e., our surgery biller) only to be subsequently reinstated. Low-volume service lines were closed or reconfigured.
Communication, once again, became a critically important part of the process. Rumors flew amongst the hospital staff, the local news, patients, other hospitals, and neighbors. Damage control again became important, especially since early advertising had been all about how the hospitals would close if the sale fell through. Fortunately, cash flow improved with receipt of deposit money from Prime and additional state funds.
DCHS filed suit against SEIU and Blue Wolf in Superior Court. Among the complaints were breach of contract for violating the confidentiality clauses, unfair competition by discouraging potential bidders, civil conspiracy for taking action that caused harm to DCHS, and aiding and abetting when Blue Wolf allowed SEIU to influence competing bidders.*
In response, the Attorney General’s office issued this press release, blaming Prime for breaking the deal. Her comments raised concerns that the conditions placed on any other sale would be the same or even more restrictive. These concerns were only slightly appeased when Attorney General Harris stated that “the offer made to Prime was unique and tailored to Prime,” and that conditions for a different transaction would not necessarily be the same.
 Back to square 1 (or maybe 2).
Back to square 1 (or maybe 2).
Within two weeks of the announcement that Prime refused the deal with the Attorney General’s conditions, our agents were again fielding requests from interested parties. The process was the same as before, so much of the work was already done. Our financial situation had slightly improved, and we updated the prospectus. Once again, we engaged in discussions with the Attorney General’s office, and with officials in Paris and Rome, so that when we had a potential buyer we would be able to move in an expedited fashion.
My mother and her neighbors who live within half a mile of the hospital sent letters to Santa Clara Supervisor Ken Yeager and San Jose Councilman Pierluigi Oliverio. They emphasized that the county would suffer a decline in tax revenue and other negative financial implications if businesses (physician offices) moved away from the area when O’Connor became “Valley North.” They asserted that property values would decline in one of the oldest, exclusive neighborhoods in San Jose. No response was received, and both Yeager and Oliverio remained remarkably silent on the entire situation.
The selection committee was reconstituted, with the addition of Sister Margaret Keaveney, who had been named the CEO of O’Connor Hospital after the planned departure of the prior CEO. It turned out that the original committee had no direct representation from the hospitals. Some observers felt that such representation might have improved the bid process and timeline.
After mostly behind-the-scenes machinations, an announcement was made on July 17, 2015, that the selected buyer would be Blue Mountain Capital in conjunction with Integrity Healthcare. The former would provide the capital and the latter the management. Key provisions of the plan included maintaining the hospitals as non-profits for at least three years, keeping them open for at least five years, and conversion of the “church plan” retirement fund to an ERISA-compliant fund.
Both parties had been involved in the original bid. Integrity had been one of the finalists, but had been unable to secure funding in a timely manner. This new combination afforded each the opportunity to play to their strengths. The management team, with whom we would be working, was comprised of executives with extensive experience in California managing both community and academic hospitals.
The paperwork was submitted to the Attorney General’s office on July 31. This meant that the 105th day allotted for public review landed on Friday, November 13. Open hearings were scheduled for the second week in October, and they were much shorter and less contentious. SEIU was remarkably quiet. The final announcement from the Attorney General’s office was made, after a short extension, on December 3. The conditions were as expected, and were accepted by Blue Mountain/Integrity.

On December 14 at 10 am, the formal transfer took place, and we became Verity Healthcare.
______________________________
*Media references to the lawsuit:
http://sternburgerwithfries.blogspot.com/2015/03/seiu-uhws-dave-regan-and-blue-wolf.html
http://www.modernhealthcare.com/article/20150225/NEWS/150229929
http://www.wsj.com/articles/when-unions-trump-hospitals-1426721146
http://www.mercurynews.com/news/ci_29250106/daughters-of-charity-health-system-closes-deal-with-hedge-fund